 Cataracts are part of the natural aging process. Everyone gets them to one degree or another if they live long enough. Cataracts, as they progress, create...
Cataracts are part of the natural aging process. Everyone gets them to one degree or another if they live long enough. Cataracts, as they progress, create...

That Depends On The Option You Choose
Should you pay extra for cataract surgery? Many surgeons refer to these options as “Premium,” “Advanced,” “Custom” or “Refractive” cataract surgery.
First let me describe the three basic choices that are available today.
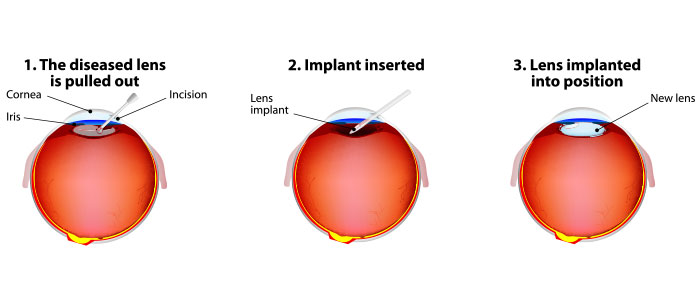
Option 1 - Basic cataract surgery
Basic surgery is what we have been doing for the last 30 years. The cataract is removed through a small incision in the eye, in almost all cases with the assistance of an instrument called a phacoemulsifier. This is an ultrasound-driven instrument that breaks the cataract into small pieces before it is then sucked out of the eye.
Once that is completed an intraocular lens is placed in the eye. This lens is called a fixed-focus lens, which means the lens allows you to see well in one place in space. Most of the time the lens is chosen for good distance vision (but it can be chosen for good near vision instead).
With this lens you see well at the distance chosen but can’t see well at other distances unless you use glasses. The other issue with this lens is if you have significant astigmatism you will still need glasses to correct that astigmatism at all distances (even the distance you chose to have the lens focused).
Option 2 - Cataract surgery and astigmatism correction
In this surgery, the cataract is removed as in the basic surgery but the surgeon is also going to do something to correct your astigmatism. There are three ways to accomplish this:
- You can make cuts in the cornea by hand.
- You can use a laser to make cuts in the cornea.
- You can insert a special implant, called a toric lens, to correct the astigmatism.
In some cases of severe astigmatism, it might be necessary to combine several of these approaches.
In this option the person would end up with good distance vision but would definitely need glasses for close-up tasks like reading.
Option 3 - An extended-range implant
For this surgery there will be a special implant inserted that tries to give you more range of focus without always needing to put glasses on.
Generally in this surgery the surgeon will also try to correct any astigmatism to give you the best chance of seeing well without glasses. When we talk about zones of vision we usually break it up into three categories: distance, intermediate (computer, card playing, playing pool), and near (reading).
Our current armamentarium of lenses is good but it is not the same as having a 20-year-old’s eyes again. Most of the implants in the extended-range implant category do well at two but not all three of the visual zones. Most people picking this option will be able to get through about 90% of their day without using glasses.
In the U.S. there are two types of extended-range implants - accommodating lenses and multifocal lenses.
The accommodating lens gives you good distance vision, fairly good intermediate vision but is a little weak with close-up reading.
The multifocal lenses split your focus into two places - one is distance and then the second focus is either intermediate or near.
There are pluses and minuses to each of the choices and the decision of which one or which combination is best for you should be decided after a discussion of your visual needs and desires with your surgeon.
The Decision
Now that I have outlined the choices, there is still the question of should you or should you not go for them.
Remember, this decision is mostly an economic one. Do you want to spend the money to be able to be LESS dependent on glasses? Notice I specifically said LESS dependent, not FREE of glasses? If anyone is promising that you will be free of glasses, it should make you think twice.
Although some people will be able to function glasses-free it is inappropriate and less than honest to tell you that you will definitely be free of glasses.
First let’s look at option 2, astigmatism correction. If you have significant astigmatism (in my view 1 diopter or greater) fixing the astigmatism will result in improved clarity of vision in almost all circumstances, so if you can at all afford it I recommend you go for that fix.
Option 3 is a bit more complex. For example, if you have other underlying eye diseases - especially Macular Degeneration, Diabetic Retinopathy or significant Glaucoma - an extended-range implant might not be recommended. With those diseases, you are generally not going to get enough benefit out of the new lenses to justify the cost. If you have no other eye disease and you can afford these new lenses, they do allow you to function at a significantly greater range of distances without glasses than the fixed-focus lenses do.
One thing you may have noticed that is missing from the discussion so far is the new option of a laser to assist in the removal of the cataract.
The latest development in cataract surgery is the use of a Femto second laser to do PARTS of the cataract surgery (the majority of the surgery is still done by hand). Although many surgeons do use the Femto second laser when they are correcting astigmatism or implanting extended-range implants that is not what you are paying extra for.
In fact, asking you to pay extra just for the use of the laser is against Medicare and many other insurers' rules and policies. Cataract surgery is considered a “covered service” and you cannot charge extra for a covered service because you are using a different machine. The only way you can charge extra for cataract surgery is if you are correcting astigmatism or presbyopia, because surgical correction of these problems are “non-covered services”.
In conclusion, if you want to be able to do more visual tasks without constantly having to reach for your glasses, you don’t have any other significant visual disease and the costs your surgeon is charging for the additional services are within your ability to pay then, yes, you should consider paying extra when you need cataract surgery in order to take full advantage of what our modern technology can do.
One last caveat: These added services are OPTIONS, not necessities. You should not be “bullied” into paying for them. If you feel like you are having your arm twisted or the office is acting more like a used car salesman than an advocate for your health get another opinion before you agree to do anything.
Article contributed by Dr. Brian Wnorowski, M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

